

|
|
Of all the surgical procedures currently performed on patients with cerebral palsy, selective dorsal rhizotomy (SDR) has undergone more thorough scientific scrutiny than any other (including orthopaedic). Accumulated evidence and our own experience indicate that SDR is an excellent option for selected patients with spastic CP. We believe parents and patients should inquire about SDR as a part of the management of CP before the patient undergoes orthopedic surgery. Outline of the SDR procedure
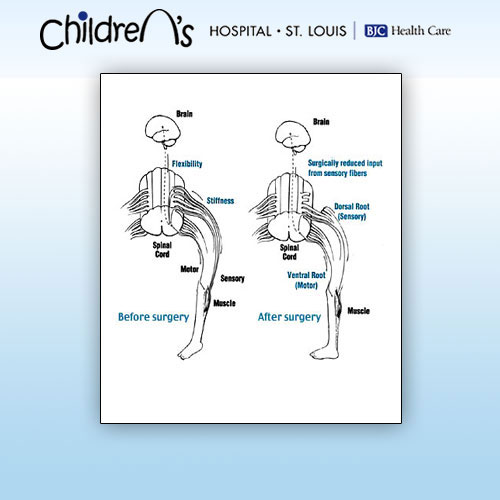
SDR involves sectioning (cutting) of some of the sensory nerve fibers that come from the muscles and enter the spinal cord.
Two groups of nerve roots leave the spinal cord and lie in the spinal canal. The ventral spinal roots send information to the muscle; the dorsal spinal roots transmit sensation from the muscle to the spinal cord.
At the time of the operation, the neurosurgeon divides each of the dorsal roots into By examining electromyographic (EMG) responses from muscles in the lower extremities, the surgical team identifies the rootlets that cause spasticity. The abnormal rootlets are selectively cut, leaving the normal rootlets intact.This reduces messages from the muscle, resulting in a better balance of activities of nerve cells in the spinal cord, and thus reduces spasticity.
Details of our SDR procedure
Different surgical techniques are utilized to perform SDR. Neurosurgeons typically perform SDR after removing the lamina ( laminectomy ) from 5-7 vertebrae. That technique was also used at our Center to perform SDR on over 140 children with CP. However, we were concerned about possible problems that can arise from removal of such a large amount of bone from the spine. Additionally, because of the extensive removal of the bone, we could not offer SDR to children with weak trunk muscles or to adults.
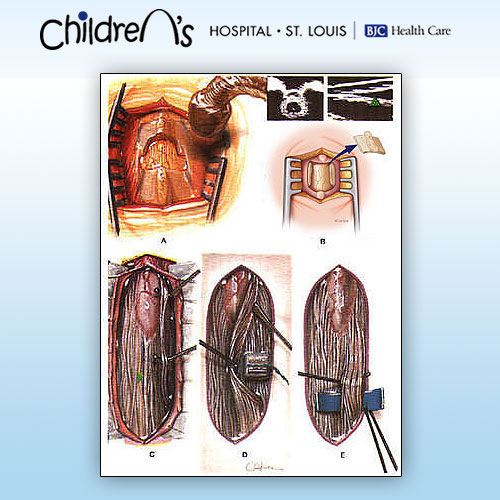
In 1991, we developed a less invasive surgical technique, which requires removal of the lamina from only 1-2 vertebrae. We refined the technique further and currently remove the lamina from a single lumbar vertebra (Figure A&B).
SDR begins with a 1- to 2-inch incision along the center of the lower back just above the waist. The spinous processess and a portion of the lamina are removed to expose the spinal cord and spinal nerves. Ultrasound and an x-ray locate the tip of the spinal cord, where there is a natural separation between sensory and motor nerves. A rubber pad is placed to separate the motor from the sensory nerves. The sensory nerve roots that will be tested and cut are placed on top of the pad and the motor nerves beneath the pad, away from the operative field.
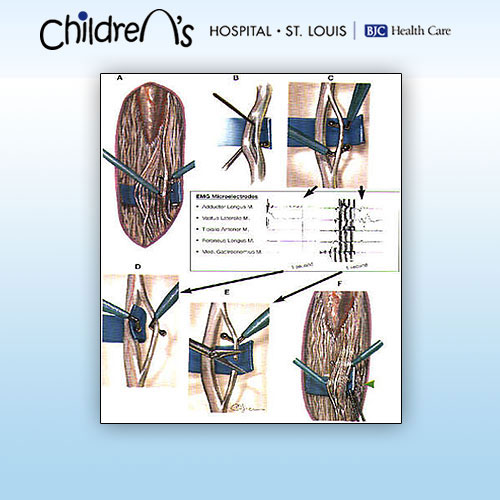
After the sensory nerves are exposed, each sensory nerve root is divided into 3-5 rootlets. Each rootlet is tested with EMG, which records electrical patterns in muscles . Rootlets are ranked from 1 (mild) to 4 (severe) for spasticity. The severely abnormal rootlets are cut. This technique is repeated for rootlets between spinal nerves L2 and S2. Half of the L1 dorsal root fibers are cut without EMG testing.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
When testing and cutting are complete, the dura mater is closed, and fentanyl is given to bathe the sensory nerves directly. The other layers of tissue, muscle, fascia, and subcutaneous tissue are sewn. The skin is closed with glue. There are no stitches to be removed from the back. Surgery takes approximately 4 hours. The patient goes to the recovery room for 1-2 hours before being transferred to the intensive care unit overnight.
Advantages of our technique over other techniques for SDR
We believe that our SDR procedure has these significant advantages over others:
- Reduced risk of spinal deformities in later years
- Decreased post-rhizotomy motor weakness
- Reduced hip flexor spasticity by sectioning the first lumbar dorsal root
- Shorter-term, less intense back pain
- Earlier resumption of vigorous physical therapy